65 yr old male with right LL consolidation
A 65 yr old male came to hospital with c/o
- breathlessness since 4 days.
- fever since 4 days.
- cough since 3 days.
HOPI -
Patient was apparently asymptomatic 4 days back, then he developed breathlessness which is insidious in onset, not associated with wheeze, increased on execution, orthopnea present, relieved with rest.
HR also c/o fever since 4 days, not associated with chills, evening rise of temperature present
He also c/o cough since 3 days, non - expectorant, increases on exposure to cold air.
C/o loss of weight, loss of appetite present, biomass exposure +.
No c/o chest pain, chest tightness, hemoptysis, palpitations, decreased urine output.
Past History :
N/k/c/o HTN, DM, epilepsy
Past h/o similar c/o SOB in winter season and usage of inhaler in the season occasionally (SOS).
No past h/o TB, covid 19
Personal history :
Loss of appetite +
Sleep - inadequate.
Occupation - farmer
Bowel and bladder g revular
Alcohol - regular 90ml/day daily
Smoking - beedis 2-3/day for 25 yrs, stopped 4yrs back.
Family history g not significant
General examination :
Patient is c/c/c tin built and moderately nourished.
No pallor, icterus, cyanosis, clubbing, Lymphedenopathy or oedema.
Temp - 99. 2 'F
PR - 98bpm
BP - 130/80 mmhg.
Sp02 - 93%.
GRBS - 78mg%.
CVS - S1 S2 +, no murmurs
RESPIRATORY SYSTEM
- dyspnoea +, Trachea - central, NVBS
Crepts present in Rt SSA, ISA, infra SA, I A, left infra SA.
Inspection :shape of chest - elliptical
Trachea - central
Expansion of chest equal on both sides
RR G 32 cpm
No usage of accessory muscles of resp
No dropping of shoulder
No crowding of ribs
No wasting of muscles
Spinoscapular distance equal on both sides
Palpation :
All inspectory findings confirmed
No local rise of temp
No tenderneaa
Apex beat in left 5th ICS medial to mid clavicular line
Percussion:
Direst - resonant
Indirect - resonant.
Auscultation :
Crepts + Rt SSA, USA, infra SA, ICA, left infra SA
P/A: soft, Non tender
CNS - NAD
Investigations on 15/5 22
Hb- 9.4gm%
TLC - 13,200
N/L/E/M - 67/27/1/5
PLT - 1.5 lakh
BT - 2min, CT - 5min
BGT - B +ve
Serology HBsAg, HIV - negative
HCV - positive
RFT :
urea-101,
Creatinine - 1.7
Uric acid - 8.8
Ca- 10, Ph - 4.7, Na- 141, K- 4.2, Cl- 99
LFT :
TB-0.67, DB - 0.2,
SGOT - 39, SGPT - 35, ALP - 119
TP - 5.5, Alb - 2.5, A/G - 0.84.
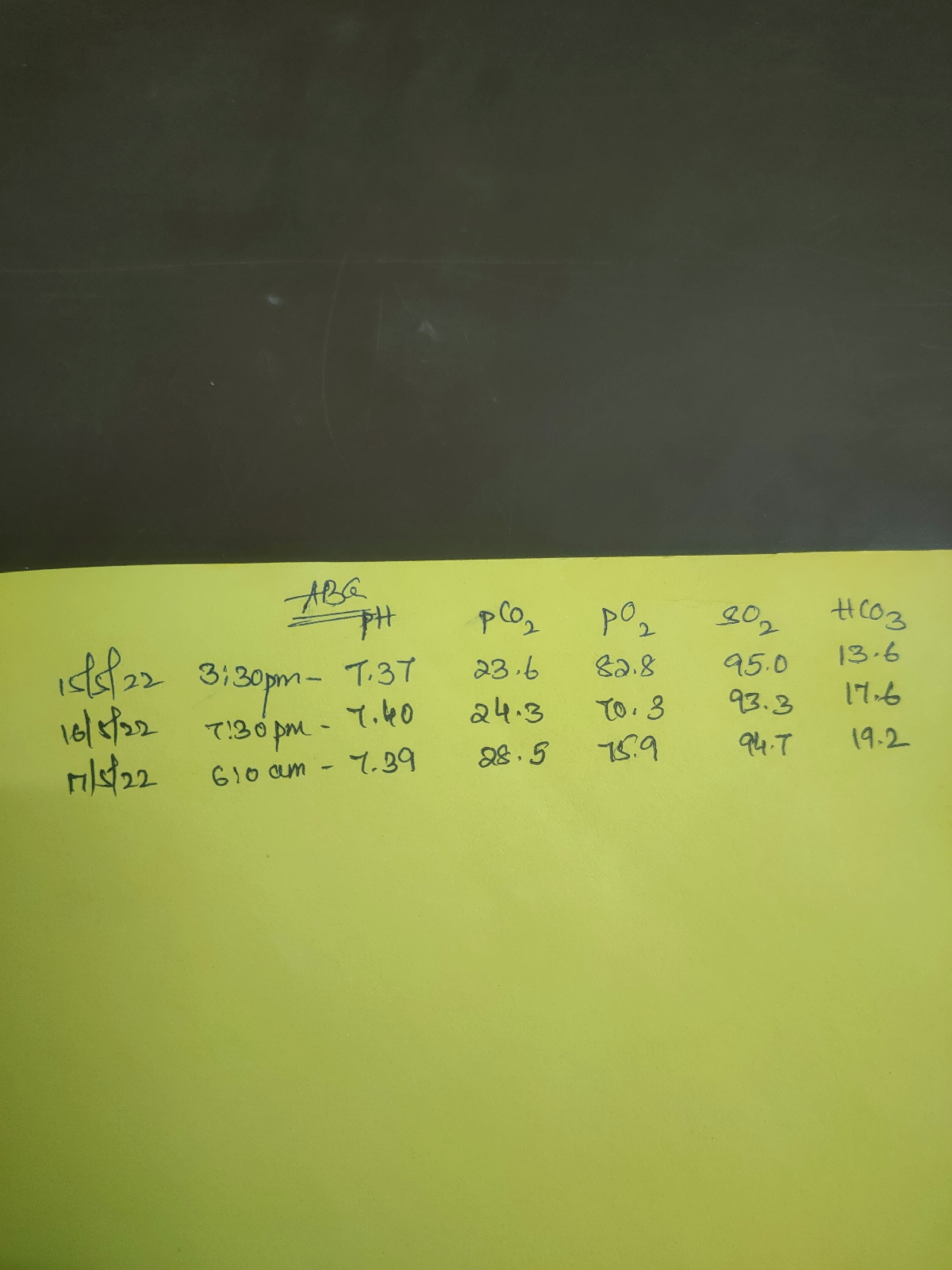
ABG-
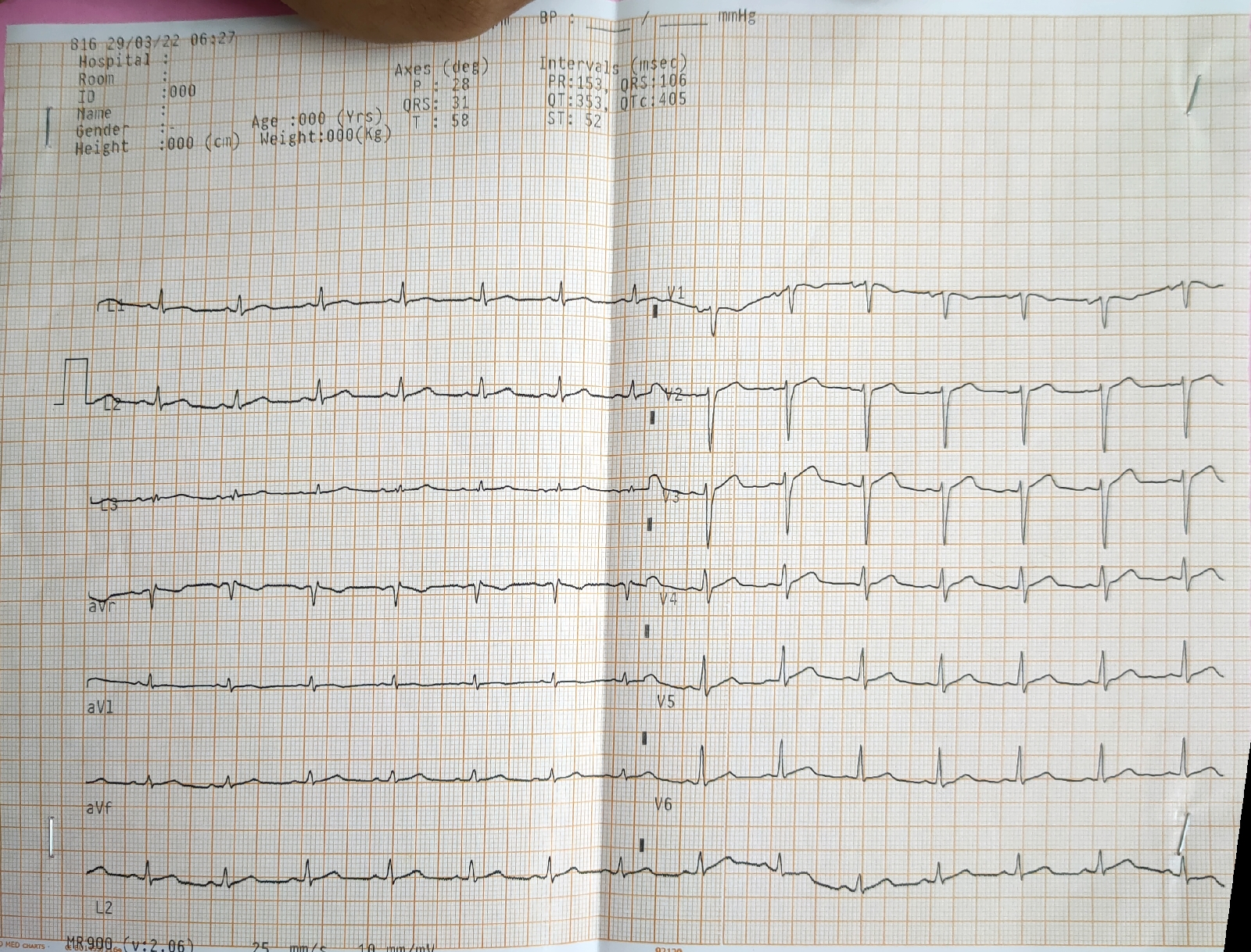
ECG-

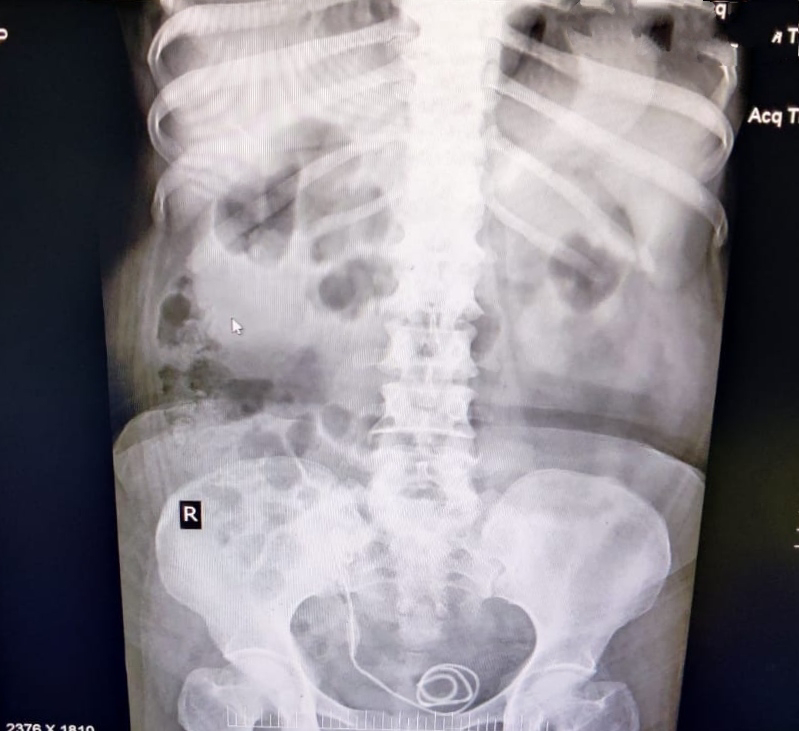
USG-

2D ECHO-

Diagnosis-Right LL consolidation 2` to? CAP,? TB with CKD
Treatment -
1.O2 with nasal prongs @2-3 lit/min
2. IVF 1unit NS @ 50ml/hr
3.Inj AUGMENTIN 1.2 gm IV /TID
4.TAB AZEE 500mg PO/OD
5.Neb with Duolin - 6th hrly, mocomist - 2nd hrly
6. Inj PAN 40mg OD BBF
7. TAB MUCINAC Ab TID
8.SYP ASCORIL 2tsp TID
9.TAB PCM 650mg BD
10. INJ NEOMOL 100ml IV /STAT